





[미숙아에게 흔한 질병①]
질병 이야기를 볼때마다 마음 한구석이 섬뜩해지고 괜한 걱정이 되는건 어쩔수 없나봅니다. 하지만, 모르고 있는것보다는 알고 미리 대처하는게 훨씬 낫겠다는 생각에 자료를 정리해서 올리겠습니다. 대부분 퍼온 내용이지만 아이가 커나가는동안에 겪은 내용이 있으면 첨부하겠습니다.
[황달]
황달이 뭐에요?
황달이란 혈액 안에 "빌리루빈"이라고 하는 것이 많아져서 피부 색이 노랗게 변하는 것을 말합니다.
빌리루빈이 뭐에요?
빌리루빈이란 혈액 안에서 산소를 실어 나르는 세포, 즉 적혈구가 깨져서 생긴 것입니다. 정상적인 경우에는 간에서 걸러져서 장으로 내와 대변으로 배설됩니다. 이것은 노란 색깔을 띄는데, 대변이 황갈색을 띄는 이유는 이 빌리루빈 때문입니다.
아기에게 황달이 왜 생기나요?
아기들의 적혈구는 어른의 적혈구보다 수명이 짧습니다. 수명이 다란 적혈구는 모두 빌리루빈으로 분해가 되서 간에서 대사가 됩니다
그런데, 미숙아는 인체의 장기가 미처 충분히 성숙되지 못해서 간이 빌리루빈을 모두 처리하지 못할 수 있습니다. 또 빌리루빈을 배출할 장도 움직임이 원활하지 못할 수 있습니다. 그러면 간에서 처리되고 장에서 배출되어야 할 빌리루빈이 혈액 안에서 축적되어서 농도가 올라갈 수 있습니다. 그러면 황달이 생길 수 있는 것입니다.
빌리루빈이 높으면 나쁜가요?
빌리루빈이 조금 올라가는 것은 아기에게 해가 되지 않습니다. 그러나 빌리루빈 치가 너무 높아지면 뇌가 손상받을 수 있기 때문에 위험합니다. 때문에 황달이 있으면 즉각 빌리루빈 치를 측정하고, 이것이 높으면 빌리루빈을 위험하지 않은 농도로 낮추기 위한 치료를 시작하게 됩니다.
황달은 어떻게 치료하나요?
빌리루빈 치가 너무 높으면 치료를 시작하는데, 대개 광선치료 방법부터 시작합니다. 이것은, 아기에게 빛을 쪼여 주는 것입니다. 이 치료법은 과거에 햇살을 드는 창가에 누운 아이들은 황달이 좋아지는 것이 우연히 발견된 후에 개발된 치료법입니다. 빛은 피부 속의 빌리루빈을 분해해서 배출되도록 합니다. 이 치료를 시작하면 설사를 할 수도 있습니다.
이 외에 빌리루빈 치가 뇌손상을 일으킬 정도로 많이 높고 광선치료에 효과가 없으면 혈장교환이라고 하는 치료를 할 수도 있습니다. 혈장이란 것은 혈액에서 세포를 뺀 물 성분을 말하는 것인데 빌리루빈은 여기에 포함되어 있습니다. 혈장교환은 이것을 걸러서 버리고 다른 사람의 혈장으로 교체함으로써 빌리루빈을 희석시키는 방법입니다.
광선치료를 할 때 아기의 눈은 왜 가리나요?
눈이 부시는 광선을 눈에 계속 쪼여주는 것은 눈에 나쁠 수 있습니다. 그래서 눈을 가리는 것입니다.
황달은 얼마나 오래 가나요?
황달이 얼마나 오래 지속될 지는 아기들마다 다릅니다. 대개 빌리루빈 치는 아기가 태어난 후 며칠간 올라가다가 떨어집니다. 따라서 광선치료는 대개 며칠간만 필요합니다. 하지만, 일주일 이상 필요한 경우도 있습니다.
엄마의 모유를 먹는 아기는 우유를 먹는 아기들보다 황달이 조금 더 오래 지속될 수 있지만, 이것은 해가 될 정도는 아닙니다.
* 아이가 세상에 나온 다음날 면회를 갔을때 인큐베이터 위에 환하게 밝은 불빛이 있었습니다. 약간 황색빛을 띤 빛을 쬐어주고 있었는데 '황달 치료기'라고 적혀있더군요. 다른 아기들은 불을 켜놓지 않고 있는데 우리 아기만 치료받고 있으니 걱정이 좀 되긴 하더군요.
이틀인가 뒤에 면회갔을때는 치료기를 꺼놓고 있었습니다. 빌리루빈 수치가 많이 낮아졌다고 하더군요. 태변도 관장시켰다고 합니다. 위에 글 읽어보셨다면 아시겠지만 아기의 장기가 아직 성숙되지 않았다는 말이지요. 그런데 다음날 다시 치료기를 켜놓아서 걱정이 좀 되었습니다. 이거 불켜지면 걱정되고 꺼지면 마음놓이고 참. 다행히 금방 치료가 되어서 다시 껐습니다만 너무 걱정하실 필요는 없을듯 싶습니다. 대부분 황달은 (인공)햇빛만 받아도 치유가 되는듯 합니다.
참, 치료를 받을때 아기눈을 보호하느라 검은 안대를 붙여 놓았더군요. 덕분에 아기얼굴을 제대로 본건 치료가 끝난 다음이었습니다. 아직 눈뜬 모습은 못봤는데 가끔 깨서 눈을 뜨기도 한다더군요. 전 계속 눈을 감고 있는건줄 알았습니다.
자발적인 호흡이 불가능하여 집에서도
상시 인공호흡기의 도움을 받아 살아가는 아이들.
원인
크게 선천적인 경우와 후천적인 경우로 나눌 수 있고
선천적인 경우는 여러 가지 증후군에 따르는 중추성 무호흡증,
호흡근의 이상, 기도기능 이상, 출산시 양수흡입으로 인한
폐의 심대한 손상과, 뇌 손상에 따른 호흡부전 등 구조적인 문제와,
출산에 따른 후휴증이 대부분.
기타 여러 가지 원인이 있을 수 있으며,
후천적으로는 치명적인 바이러스 감염에 의한 폐렴을 앓고 난 후
폐가 손상되어 나타나는 것이 대부분.
임상증상
자발적으로 호흡을 할 수 없어 얼굴이 파래지고 가래가 심해지며
산소만 별도로 공급하여 줄 경우 이산화탄소가 체내에 축척되어
더욱 심한 호흡곤란을 겪을 수 있고, 심박이 상승하고
음식물과 타액이 기도로 흡입되어 폐의 기능을 손상시키고
보통 저항력이 약해 쉽게 감기에 걸리고 방치할 경우
심각한 뇌 손상을 일으킬 수 있습니다.
진단
일반병원에서 진단할 수는 있으나,
수술적인 치료가 되는 것이 아니기 때문에
체계적인 관리를 할 수 있는 병원이 무엇보다 중요합니다.
특히 관리 잘못으로 인한 복합장애는 아이의 인생을 망칠 수 있습니다.
현재로서는 삼성 서울병원 소아과 홈케어클리닉팀이
가장 전문화 되어있고 앞서 있다는 평가를 받고 있습니다.
치료
병원에서 장기적인 입원치료가 필요하고,
우선 인공호흡기를 사용하여 아이를 편하게 하여 주고
대신 아이가 기계에 적응되어 버리면
자발적인 호흡능력이 상실될 수 있으므로
세심한 관리와 주의가 필요합니다.
기도천공과 기도흡입으로 입으로 음식물을 먹기가 어려워
위를 직접 천공하여 특수분유를 처방 받아 공급해 주고
장기간 병원생활을 하게되면 감염위험에 노출되고
지체장애가 동반될 수 있으므로, 인공호흡기와 부대 의료장비를 구입.
집에서 엄마와 함께 생활하며 치료해 나가는 것이 아이가
빨리 호전될 수 있는 지혜로운 길입니다.
집에서 항상 감염에 주의하고 특히 감기는 아이에게는 치명적입니다.
그리고 물리치료와 언어치료 등 적절한 치료를 병행해 주어야
아이가 호흡기능을 회복하는데 도움이 됩니다.
잠시의 방심으로 치명적인 뇌손상이 올 수 있으므로
엄마의 끈질긴 인내와 노력이 필요합니다.
기관지 폐 이형성증은
미숙한 폐에 산소 독성 및 기압상해가 가해져서
폐포 및 기관지의 손상이 생기고
이의 치유과정에 이상이 초래되어
기관지, 폐포 및 폐간질에 섬유화가 남는 것으로 추정되는
만성 폐질환.
생후 첫 1 주일간 미숙아에서 주로 발생하며,
아기가 엄마 뱃속에 있었던 기간이 짧을수록,
혹은 출생시 체중이 적을수록 많이 발생.
원인은 높은 농도의 산소요법 및
보조적 환기요법에 의한 미숙한 폐포의 압력상해이나
동맥관 개존증, 폐렴, 무기폐, 비타민 A 등의 영양부족,
유전적 요인 등이 복합적으로 작용하여 발생하기도 합니다.
최근 우리나라에서도 신생아의 집중치료에 대한 질적 수준이 향상되고
기계호흡 치료에 의한 조산아들의 생존률이 증가함에 따라
그 후유증의 하나인 기관지 폐이형성증의 발생빈도가 낮아지고 있습니다.
치료가 어려우므로 예방이 중요합니다.
기관지폐이형성증이란 신생아기에 호흡곤란 증후군이나 심장 질환으로 오랫동안 산소치료와 인공호흡기를 사용했던 아기에게 생기는 만성 폐질환입니다. 장기간의 높은 농도의 산소와 인공호흡기의 높은 압력은 아이의 폐와 기도에 손상을 입힙니다. 특히 미숙아에게 이병은 생기기 쉽습니다.
이 병이 있는 아기는 숨을 빨리 쉬고 힘들게 쉬며 숨소리가 거칠고 쌕쌕거립니다. 그리고 호흡기 감염이 자주 오고 피부가 파랗게 되는 일도 생깁니다. 성장도 잘 되지 않고 먹이기도 힘듭니다. 대개의 경우 지내기 위해서는 산소가 필요한 경우가 많습니다. 임상 증상과 가슴 사진을 보면 진단을 내릴 수 있습니다.
대개 병이 좋아짐에 따라 필요로 하는 산소 농도, 압력의 양이 줄긴 하지만 손상된 폐로 호흡하기 위해서는 산소와 인공호흡기가 필요합니다. 인공호흡기를 성공적으로 떼게 되면 이후에는 마스크나 코에 연결하는 대롱을 이용하여 산소를 수주에서 수개월 동안 공급받을 수도 있습니다.
아기의 식사는 입으로 직접 할 수도 있으나 코쪽으로 튜브를 설치해 공급할 수도 있고 수술적으로 배쪽으로 튜브를 설치해 공급할 수도 있습니다. 기관지를 넓히거나 폐의 수분을 제거하는 약물 복용을 할 수도 있습니다. 수년동안 호흡기 감염 또는 신체적 활동 시 쌕쌕거리는 호흡음이 들리거나 호흡곤란을 호소할 수 있으나 나이가 들면서 병의 경과는 좋아집니다.
 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/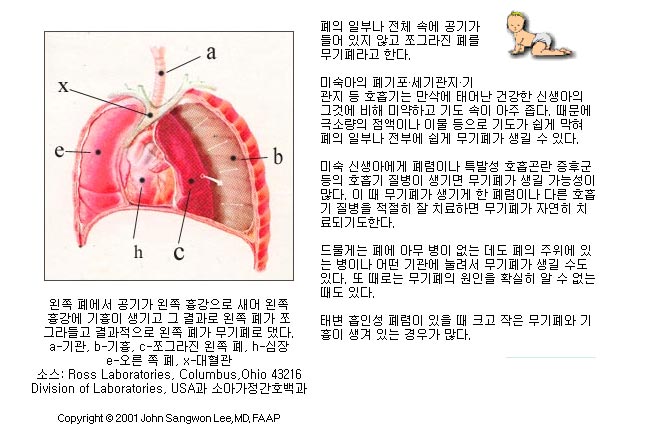 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/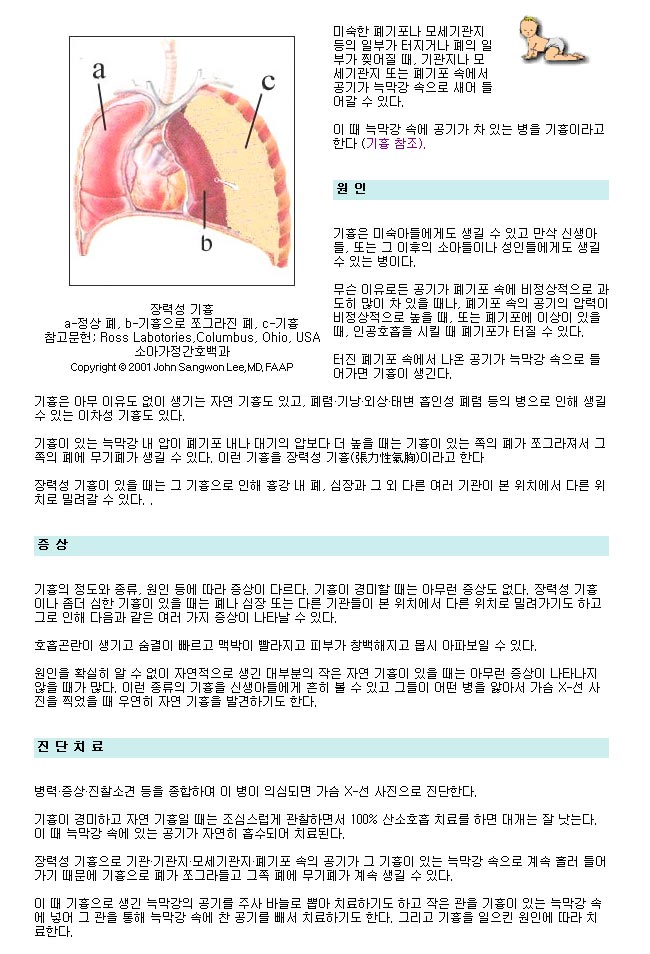 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/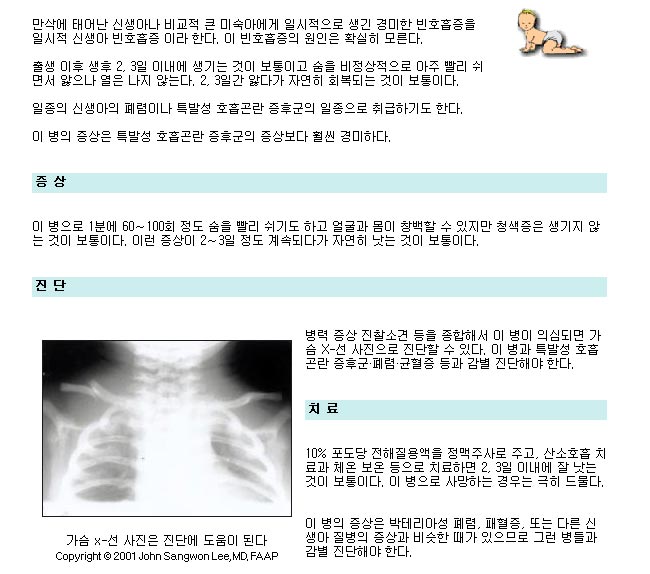 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 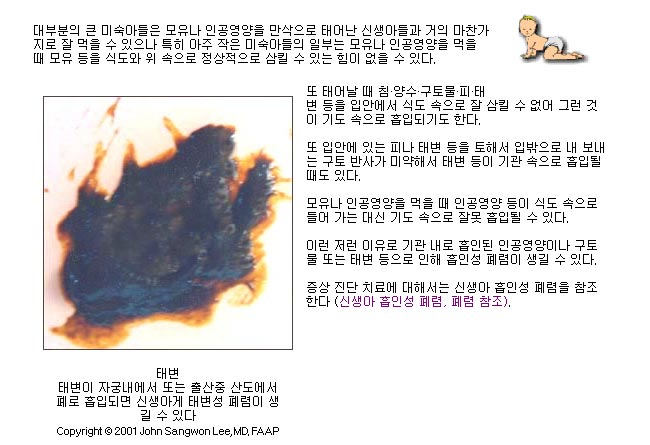 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/ 소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/
소아과 전문의 이상원의 부모도 반의사가 되어야 한다에서 발췌 - http://www.koreapediatrics.com/저희 부모들에게는 어려운 내용들 이지만, 병원에 계신 의사선생님들이나, 장차 소아과의사 선생님이 되려고 하시는 분들에게 도움이 될까해서, 인터넷을 뒤지다가 찾은 내용을 올립니다.
혹시 문서작업 하시려고 하는데, 편집이 않되는 분들은 전화주세요.^^
- 앞으로도 전문자료등도 항상 올리도록 하겠습니다. -
Retinopathy of prematurity (ROP) has been divided into five stages. Stages 1 and 2 customarily get better on their own. Some eyes, however, go on to Stage 3 retinopathy of prematurity. This happens when new blood vessels start to grow from the retina toward the center of the eye, forming a ridge between retina that has blood vessels in the back of the eye, and the retina that does not have blood vessels in the front of the eye.
This difference in the blood vessels of the retina is because the premature baby has not had the time while in the womb to allow the blood vessels within the retina to grow all the way from the optic nerve in the back of the eye to the front of the eye.
Stage 3 ROP exists when these disturbing new blood vessels grow out from the ridge in the retina toward the center of the eye. If this blood vessel growth becomes severe and is accompanied by “plus” disease, the child may reach the point where treatment of the peripheral retina with laser (or rarely freezing) treatment is performed. “Plus” disease is defined as enlarged and twisting blood vessels in the back part of the eye.
Stage 3 ROP
Stage 3 ROP exists when these disturbing new blood vessels grow out from the ridge in the retina toward the center of the eye. If this blood vessel growth becomes severe and is accompanied by “plus” disease, the child may reach the point where treatment of the peripheral retina with laser (or rarely freezing) treatment is performed. “Plus” disease is defined as enlarged and twisting blood vessels in the back part of the eye.

Plus Disease
Peripheral retinal treatment can reduce, but not eliminate, the chance of the ROP progressing to the potentially blinding stages 4 and 5. When stage 4 or 5 ROP is reached, the retina is detached and other therapies can be performed.
Stage 4 ROP
One such therapy is scleral buckling, which involves encircling the eyeball with a silicone band to try and reduce the pulling on the retina. Other therapies include vitrectomy (removal of the gel-like substance called the vitreous that fills the back of the eye). Sometimes the removal of the lens as well is required during vitrectomy to try and eliminate as much pulling as possible from the retinal surface. Removal of the lens is performed if the retina is touching the back surface of the lens, which would make it impossible to enter the eye for vitreous surgery without damaging the retina.
When scleral buckling is considered the appropriate procedure, the success rate is 70% retinal reattachment. Vitreous surgery for stage 4B, where the retina responsible for central vision is detached, or stage 5, where all the retina is detached, had a success rate of 76% reattachment. The child’s vision after these procedures were in the ranges of:
20/60 to 20/300 for 15% of eyes
20/60 to 20/800 for 30% of eyes
20/60 to 20/1900 for 48% of eyes (ambulatory vision)
light perception for 72% of eyes
Ambulatory vision is defined as being able to see objects and move around a room without stumbling or bumping into obstacles. Unfortunately, 28% of children even with appropriate management and vitreous surgery end up with no light perception.
Recently, vitreous surgery is being performed earlier, at stage 4A, where the retina responsible for central vision remains attached, and shows promise of success rates of up to 90%. Visual results in this population are not available currently, but are suspected to be perhaps better than when surgery is performed at stage 4B or 5.
The development of vision is dependent on many factors, much of which we probably don’t fully understand, but certainly issues relative to the child’s glasses needs, central nervous system development, and developing the “wiring” for vision based on competition between the two eyes are all factors that enter into the child’s final visual acuity. Fortunately, children are able to adapt to lower levels of vision and use their vision at levels much higher than what their measured visual acuity might suggest. Children with a visual acuity of 20/200, which would be classified as legally blind, very often function at a level much better than that when they are observed performing their daily tasks.
Certainly there is much progress to be made in the area of retinopathy of prematurity and other forms of pediatric retinal detachment that hopefully will yield even better visual results. Some of these things will be aided by the development of drugs that can control this new blood vessel growth, as well as developments of microelectronics and other tissue manipulation techniques.
In December of 2003, the results of the Early Treatment Retinopathy of Prematurity Study were released. They showed that treating eyes that are vascularly active with plus disease and with changes of ROP in zone 1 yielded fewer eyes going on to stages 4 and 5 (retinal detachment). The treatment performed in this study was primarily laser peripheral ablation and the eyes were treated within two days of diagnosis. This study does support earlier intervention and will reduce, hopefully, the number of children who go on to blindness from retinal detachment.
For more in-depth information on retinopathy of prematurity you can access the Physician's Education section of our website: http://www.ropard.org/learning/
Retinopathy of Prematurity (ROP)
The information provided in this Resource Guide was developed by the National Eye Institute to help patients and their families search for general information about early treatment for retinopathy of prematurity study (ETROP). An eye care professional who has examined the patient's eyes and is familiar with his or her medical history is the best person to answer specific questions.
retrolental fibroplasia
Retinopathy of prematurity (ROP) is a potentially blinding eye disorder that primarily affects premature infants weighing about 2¾ pounds (1250 grams) or less that are born before 31 weeks of gestation (A full-term pregnancy has a gestation of 38–42 weeks). The smaller a baby is at birth, the more likely that baby is to develop ROP. This disorder—which usually develops in both eyes—is one of the most common causes of visual loss in childhood and can lead to lifelong vision impairment and blindness. ROP was first diagnosed in 1942.
Today, with advances in neonatal care, smaller and more premature infants are being saved. These infants are at a much higher risk for ROP. Not all babies who are premature develop ROP. There are approximately 3.9 million infants born in the U.S. each year; of those, about 28,000 weigh 2¾ pounds or less. About 14,000–16,000 of these infants are affected by some degree of ROP. The disease improves and leaves no permanent damage in milder cases of ROP. About 90 percent of all infants with ROP are in the milder category and do not need treatment. However, infants with more severe disease can develop impaired vision or even blindness. About 1,100–1,500 infants annually develop ROP that is severe enough to require medical treatment. About 400–600 infants each year in the US become legally blind from ROP.
ROP occurs when abnormal blood vessels grow and spread throughout the retina, the tissue that lines the back of the eye. These abnormal blood vessels are fragile and can leak, scarring the retina and pulling it out of position. This causes a retinal detachment. Retinal detachment is the main cause of visual impairment and blindness in ROP.
Several complex factors may be responsible for the development of ROP. The eye starts to develop at about 16 weeks of pregnancy, when the blood vessels of the retina begin to form at the optic nerve in the back of the eye. The blood vessels grow gradually toward the edges of the developing retina, supplying oxygen and nutrients. During the last 12 weeks of a pregnancy, the eye develops rapidly. When a baby is born full-term, the retinal blood vessel growth is mostly complete (The retina usually finishes growing a few weeks to a month after birth). But if a baby is born prematurely, before these blood vessels have reached the edges of the retina, normal vessel growth may stop. The edges of the retina—the periphery—may not get enough oxygen and nutrients.
Scientists believe that the periphery of the retina then sends out signals to other areas of the retina for nourishment. As a result, new abnormal vessels begin to grow. These new blood vessels are fragile and weak and can bleed, leading to retinal scarring. When these scars shrink, they pull on the retina, causing it to detach from the back of the eye.
Yes. ROP is classified in five stages, ranging from mild (stage I) to severe (stage V):
Stage I — Mildly abnormal blood vessel growth. Many children who develop stage I improve with no treatment and eventually develop normal vision. The disease resolves on its own without further progression.
Stage II — Moderately abnormal blood vessel growth. Many children who develop stage II improve with no treatment and eventually develop normal vision. The disease resolves on its own without further progression.
Stage III — Severely abnormal blood vessel growth. The abnormal blood vessels grow toward the center of the eye instead of following their normal growth pattern along the surface of the retina. Some infants who develop stage III improve with no treatment and eventually develop normal vision. However, when infants have a certain degree of Stage III and "plus disease" develops, treatment is considered. "Plus disease" means that the blood vessels of the retina have become enlarged and twisted, indicating a worsening of the disease. Treatment at this point has a good chance of preventing retinal detachment.
Stage IV — Partially detached retina. Traction from the scar produced by bleeding, abnormal vessels pulls the retina away from the wall of the eye.
Stage V — Completely detached retina and the end stage of the disease. If the eye is left alone at this stage, the baby can have severe visual impairment and even blindness.
Most babies who develop ROP have stages I or II. However, in a small number of babies, ROP worsens, sometimes very rapidly. Untreated ROP threatens to destroy vision.
The most effective proven treatments for ROP are laser therapy or cryotherapy. Laser therapy "burns away" the periphery of the retina, which has no normal blood vessels. With cryotherapy, physicians use an instrument that generates freezing temperatures to briefly touch spots on the surface of the eye that overlie the periphery of the retina. Both laser treatment and cryotherapy destroy the peripheral areas of the retina, slowing or reversing the abnormal growth of blood vessels. Unfortunately, the treatments also destroy some side vision. This is done to save the most important part of our sight—the sharp, central vision we need for "straight ahead" activities such as reading, sewing, and driving.
Both laser treatments and cryotherapy are performed only on infants with advanced ROP, particularly stage III with "plus disease." Both treatments are considered invasive surgeries on the eye, and doctors don't know the long-term side effects of each.
In the later stages of ROP, other treatment options include:
While ROP treatment decreases the chances for vision loss, it does not always prevent it. Not all babies respond to ROP treatment, and the disease may get worse. If treatment for ROP does not work, a retinal detachment may develop. Often, only part of the retina detaches (stage IV). When this happens, no further treatments may be needed, since a partial detachment may remain the same or go away without treatment. However, in some instances, physicians may recommend treatment to try to prevent further advancement of the retinal detachment (stage V). If the center of the retina or the entire retina detaches, central vision is threatened, and surgery may be recommended to reattach the retina.
In addition to birth weight and how early a baby is born, other factors contributing to the risk of ROP include anemia, blood transfusions, respiratory distress, breathing difficulties, and the overall health of the infant.
An ROP epidemic occurred in the 1940s and early 1950s when hospital nurseries began using excessively high levels of oxygen in incubators to save the lives of premature infants. During this time, ROP was the leading cause of blindness in children in the US. In 1954, scientists funded by the National Institutes of Health determined that the relatively high levels of oxygen routinely given to premature infants at that time were an important risk factor, and that reducing the level of oxygen given to premature babies reduced the incidence of ROP. With newer technology and methods to monitor the oxygen levels of infants, oxygen use as a risk factor has diminished in importance.
Although it had been suggested as a factor in the development of ROP, researchers supported by the National Eye Institute determined that lighting levels in hospital nurseries has no effect on the development of ROP.
Yes. Infants with ROP are considered to be at higher risk for developing certain eye problems later in life, such as retinal detachment, myopia (nearsightedness), strabismus (crossed eyes), amblyopia (lazy eye), and glaucoma. In many cases, these eye problems can be treated or controlled.
The NEI-supported clinical studies on ROP include:
The Cryotherapy for Retinopathy of Prematurity (CRYO-ROP)-Outcome Study of Cryotherapy for Retinopathy of Prematurity Study examined the safety and effectiveness of cryotherapy (freezing treatment) of the peripheral retina in reducing the risk of blindness in certain low birth-weight infants with ROP. Follow-up results confirm that applying a freezing treatment to the eyes of premature babies with ROP helps save their sight. The follow-up results also give researchers more information about how well the babies can see in the years after cryotherapy. Read more about the CRYO-ROP study.
The Effects of Light Reduction on Retinopathy of Prematurity (Light-ROP) Study evaluated the effect of ambient light reduction on the incidence of ROP. The study determined that light reduction has no effect on the development of a potentially blinding eye disorder in low birthweight infants. The study determined that light reduction in hospital nurseries has no effect on the development of ROP. Read more about the Light-ROP study.
The Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity (the STOP-ROP) Multicenter Trial tested the efficacy, safety, and costs of providing supplemental oxygen in moderately severe retinopathy of prematurity (prethreshold ROP). Results showed that modest supplemental oxygen given to premature infants with moderate cases of ROP may not significantly improve ROP, but definitely does not make it worse. Read more about the STOP-ROP study.
The Early Treatment for Retinopathy of Prematurity Study (ETROP) is designed to determine whether earlier treatment in carefully selected cases of ROP will result in an overall better visual outcome than treatment at the conventional disease threshold point used in the CRYO-ROP study. Read more about the ETROP study.
The following organizations may be able to provide additional information on retinopathy of prematurity:
출처 http://www.nei.nih.gov/health/rop/index.asp

2020-06-25

2019-08-15

2019-02-06

2018-12-08

2018-11-06
 02-3667-3919
02-3667-3919
















